Emerald v3
Goal One
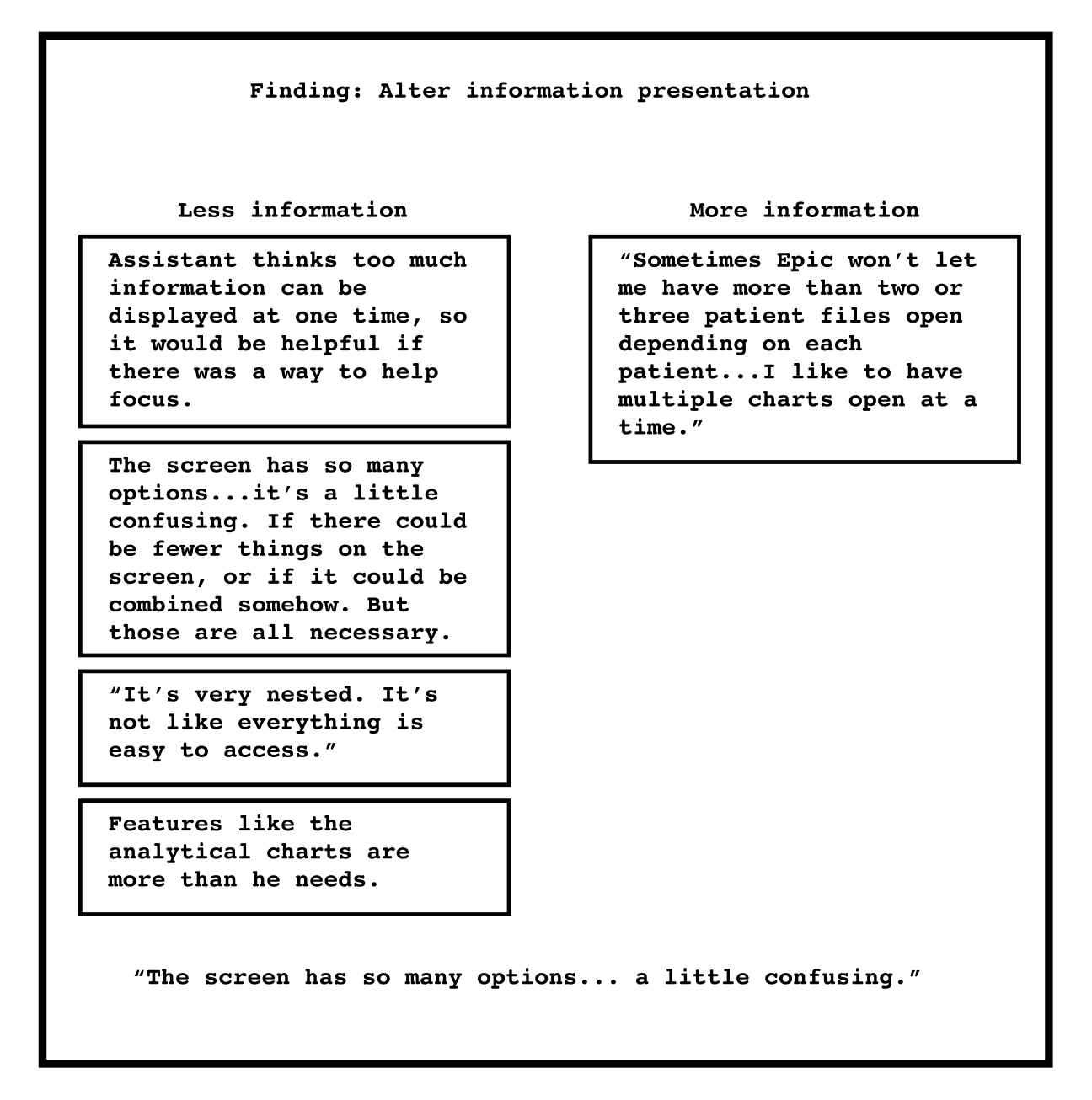
The key takeaway from the interviews was the need for less information on screen. Other interviews suggest the same as they described repetitive tasks and a drawn-out process to writing notes.
Goal Three
Exploring accessibility
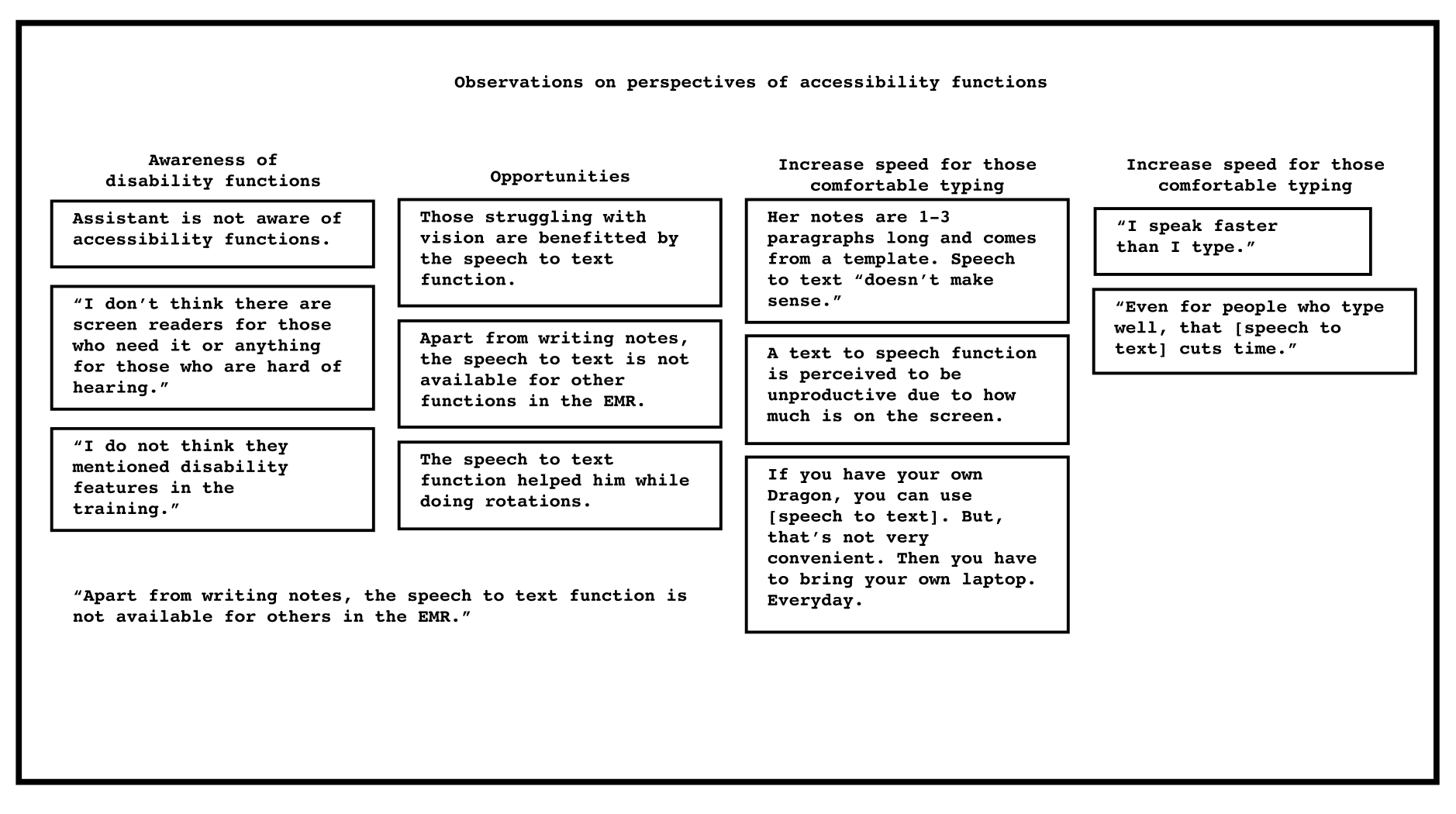
There were various opportunities noted when it came to improving or creating accessibility functions. One of primary interest were adjustments to the speech to text transcription function which is currently a popular (but expensive) add-on.
User Stories
User stories helped identify useful paths to move forward with:
- I would like to search cancer diagnoses by diagnostic codes so I can pull up presets faster.
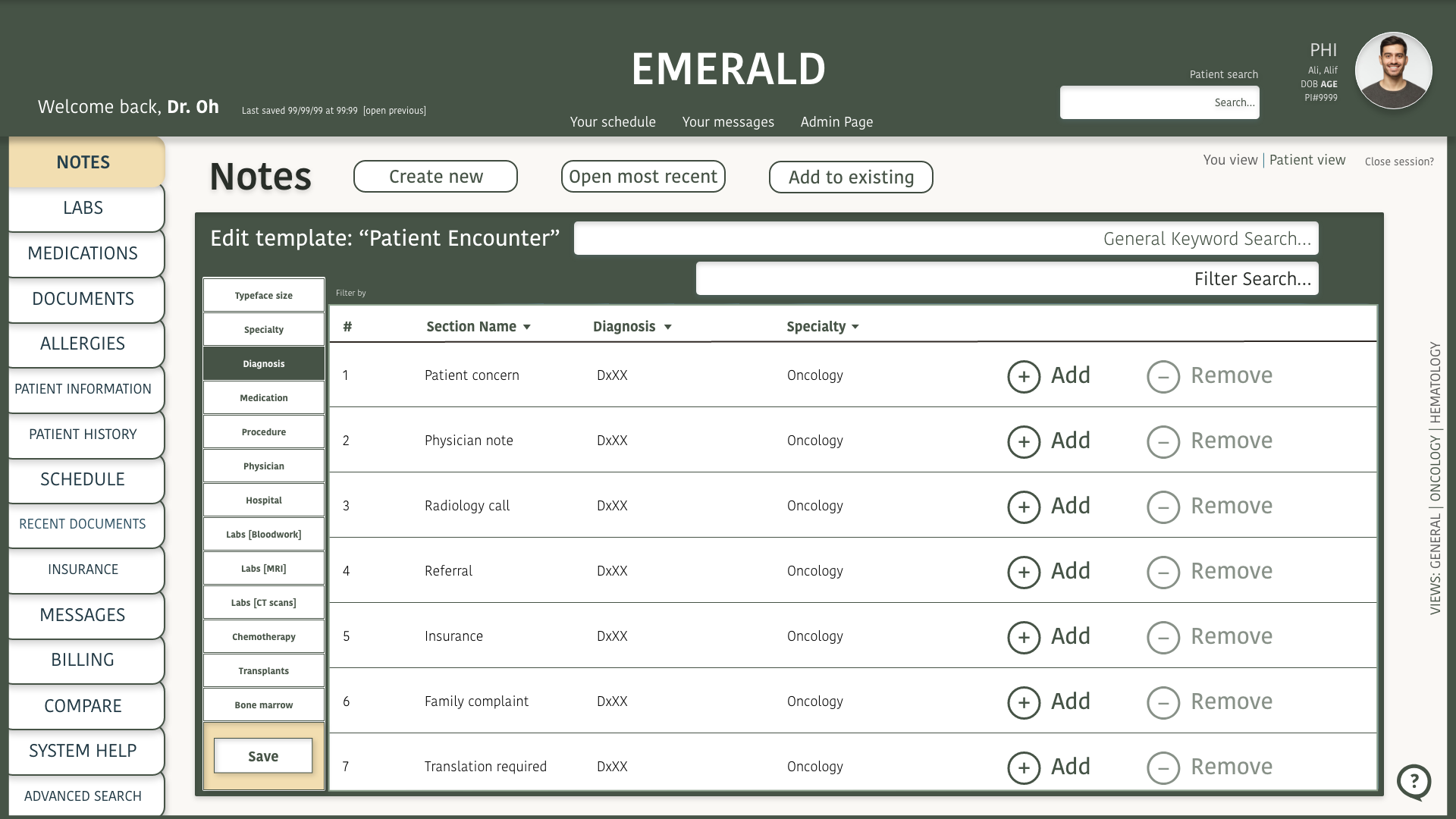
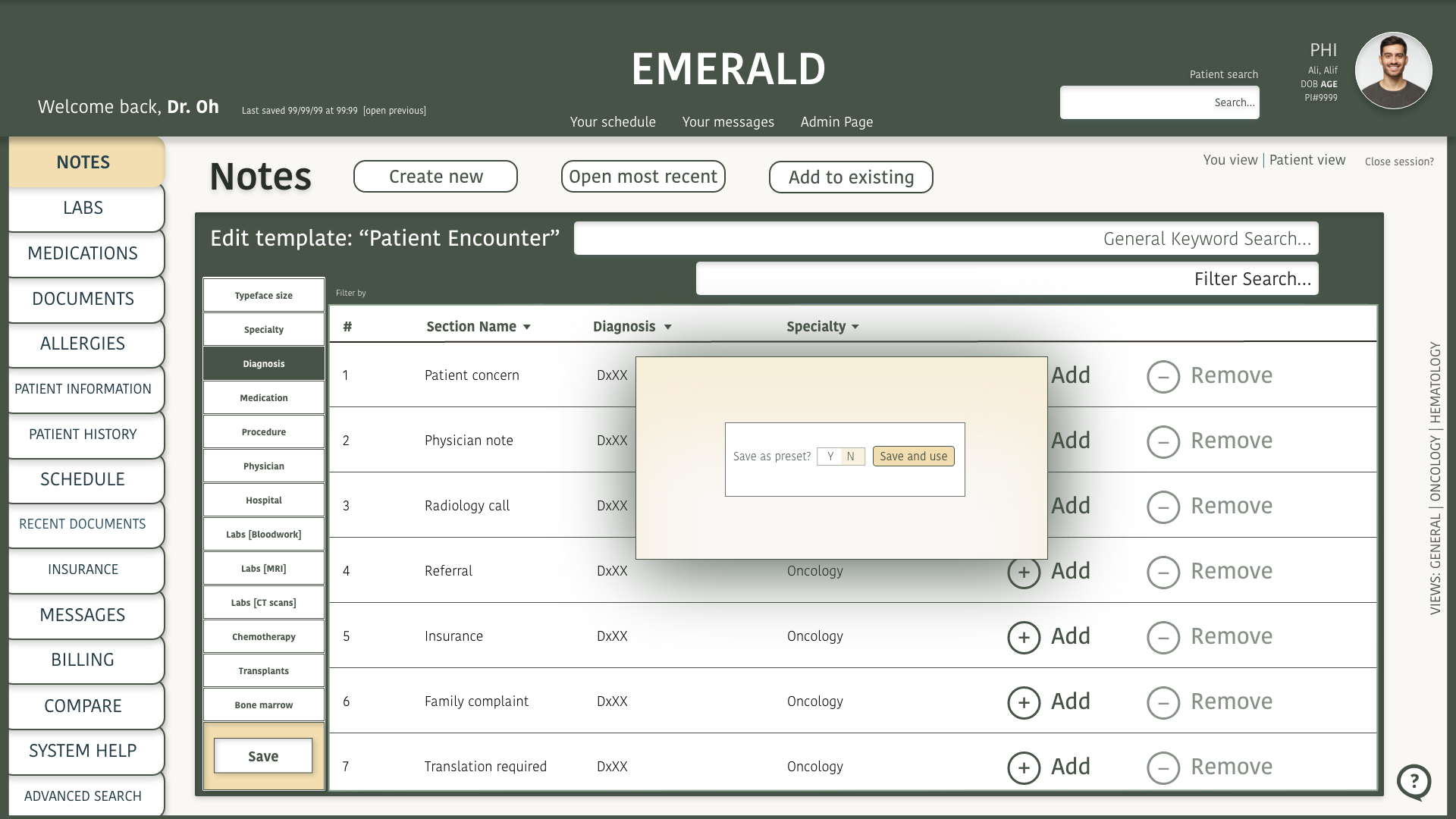
- I would like to customize presets so I can streamline my workflow.
- I would like to add note templates so I can customize my workflow.
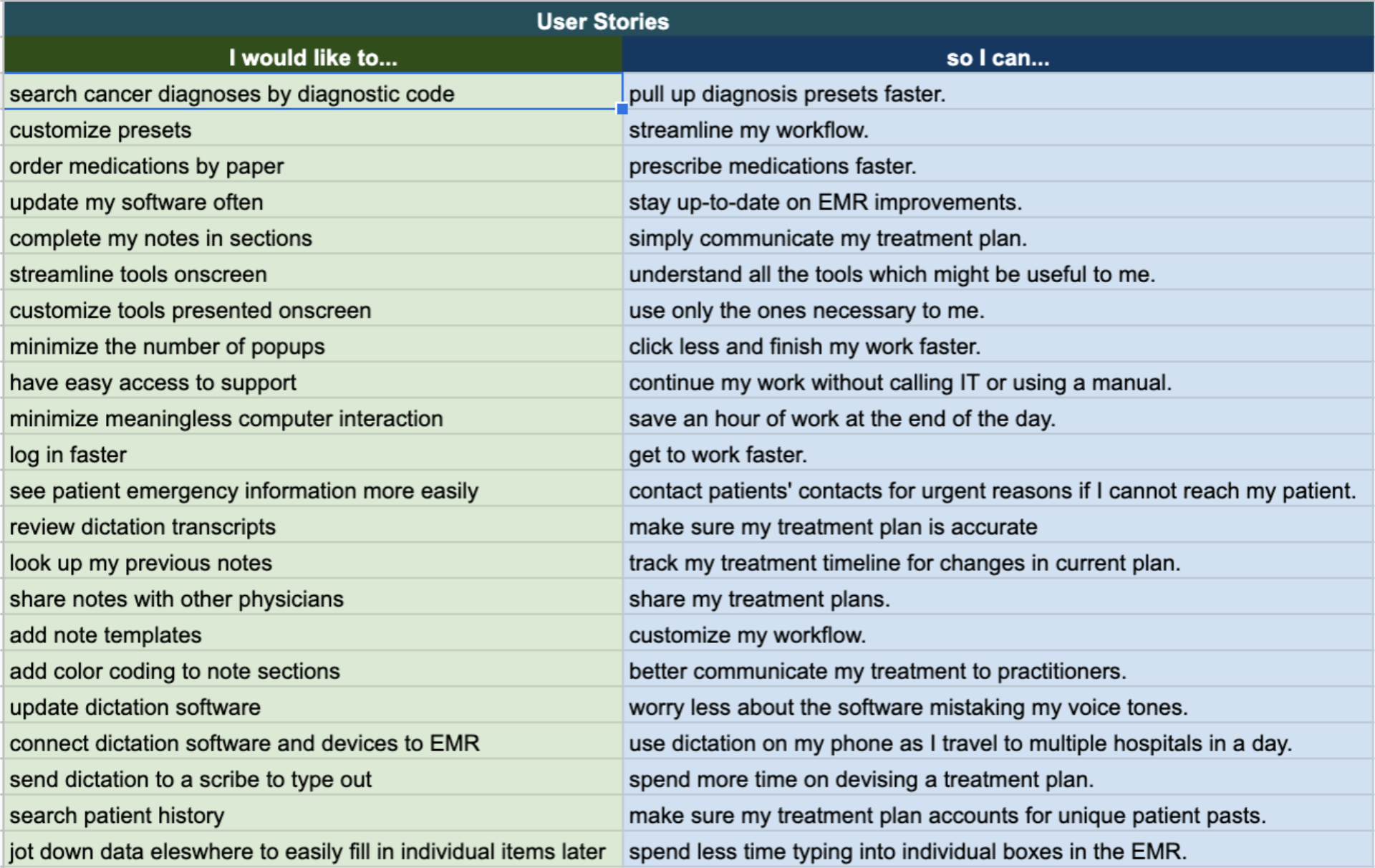
User stories helped with identifying key user flows.
Reflecting on the insights, the design problems in my scope were:
- Notes take too long to write.
- There are too many “clicks” in modern EMRs.
- There are too many features on the screen.
The general sentiment is that it feels like you can never really “win” with an EMR.
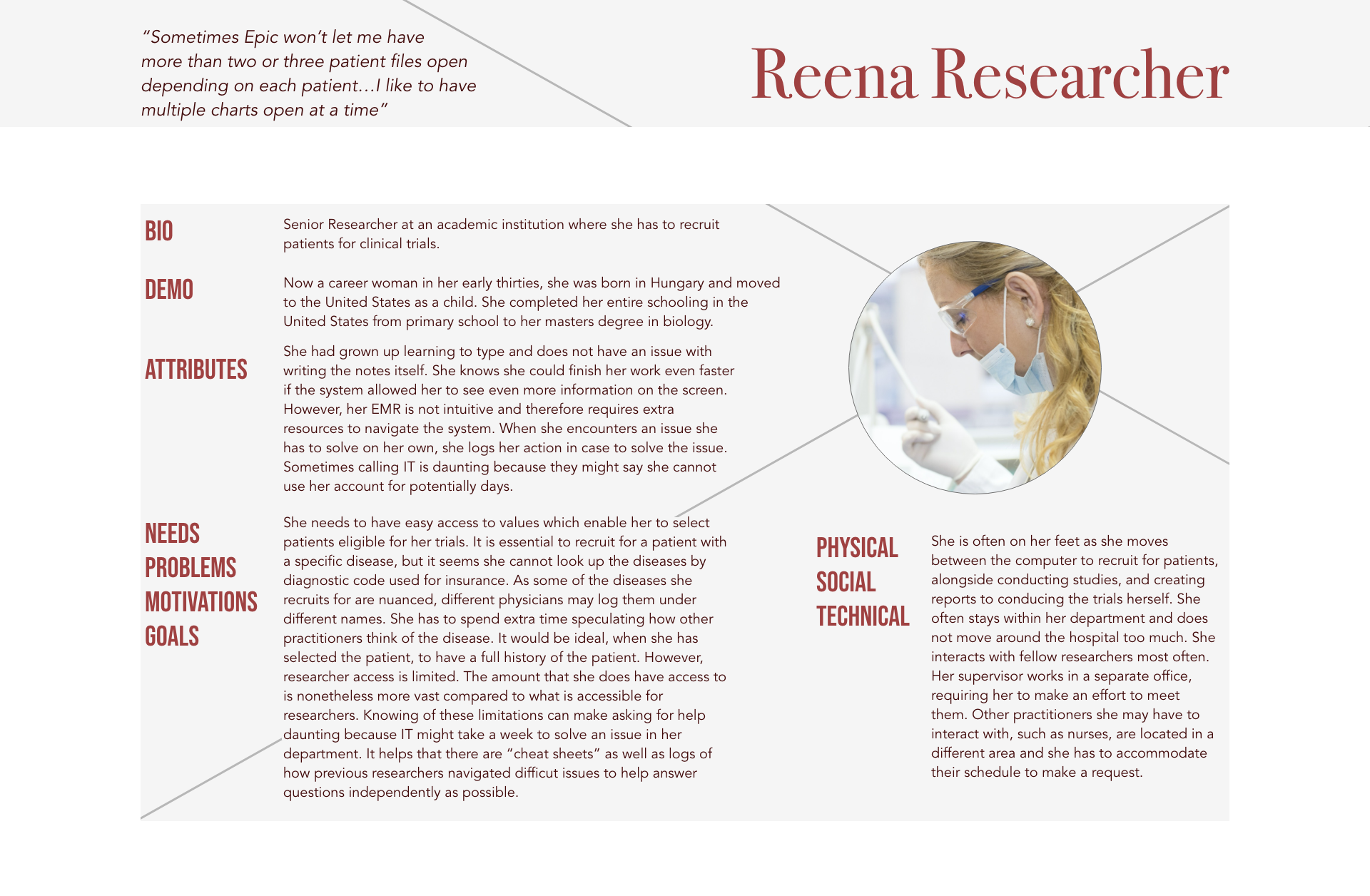
Researchers find that EMRs aren’t made for their role, despite needing to access patient data is a core function of their role.
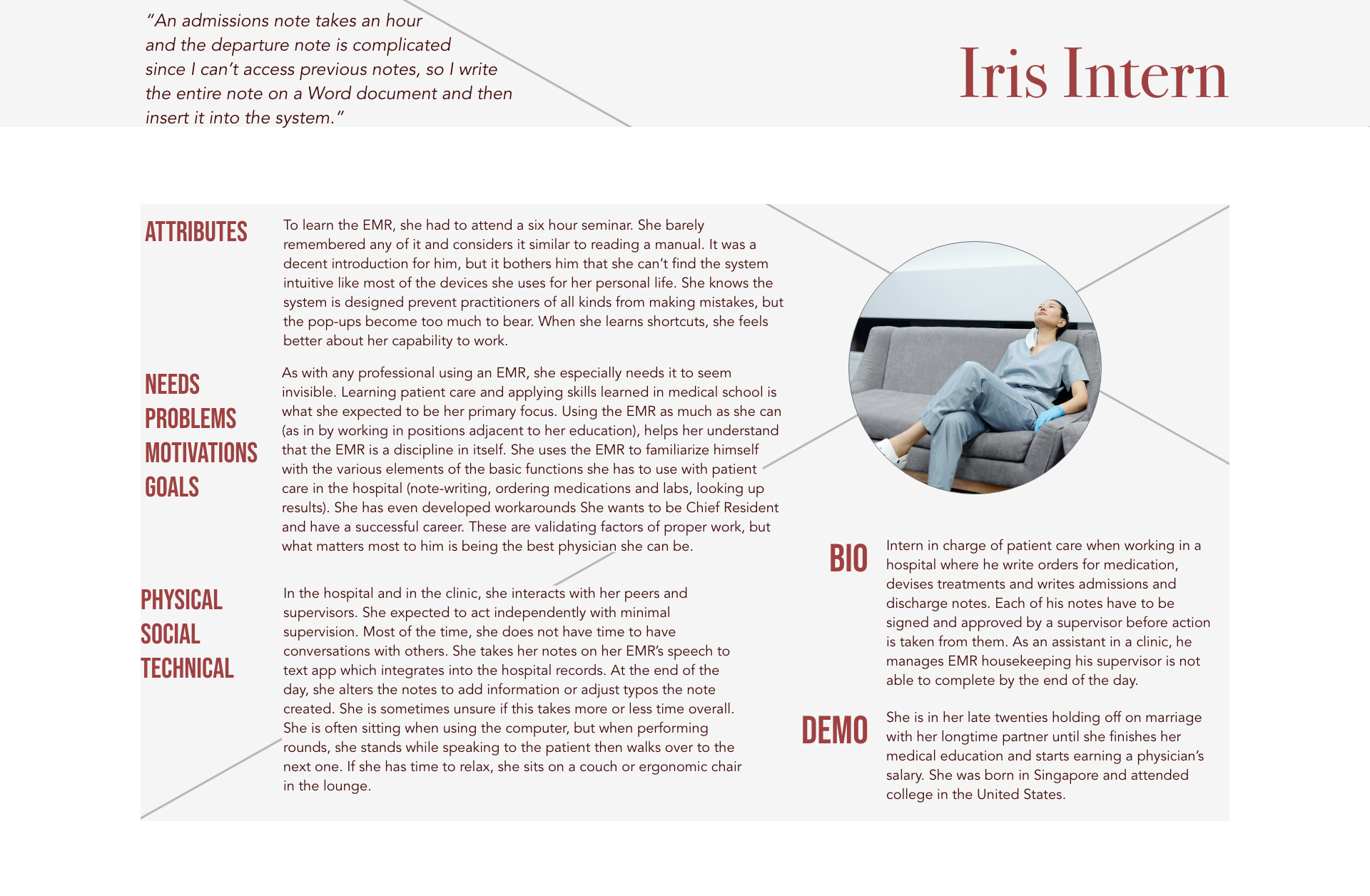
Interns working long hours find it is easier to type notes in external documents to copy into the EMR than writing in the system directly.
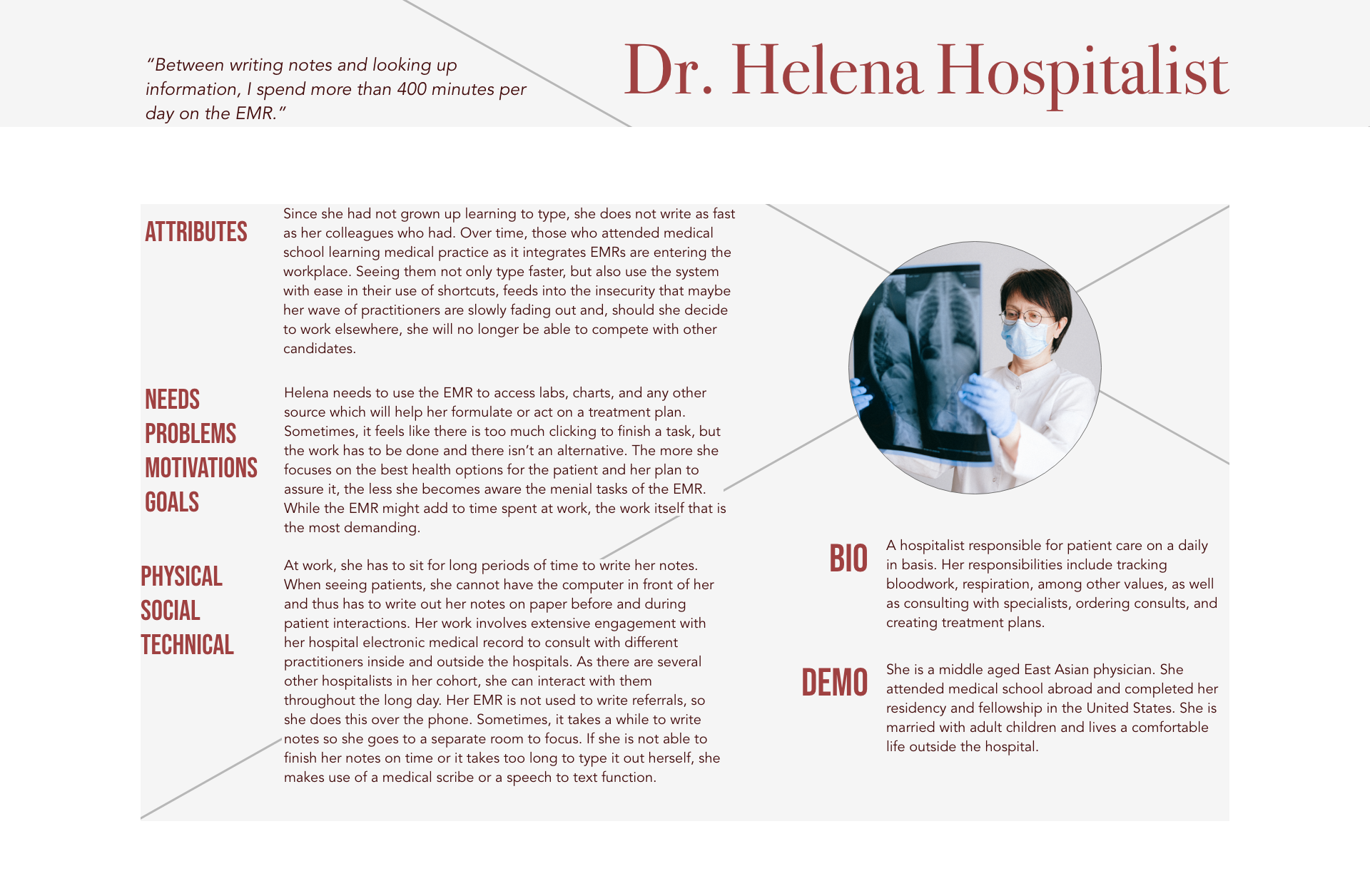
Some hospitalists tracked spending an extra 400 minutes on her work by using an EMR.
I eventually devised a new one centralizing the findings.
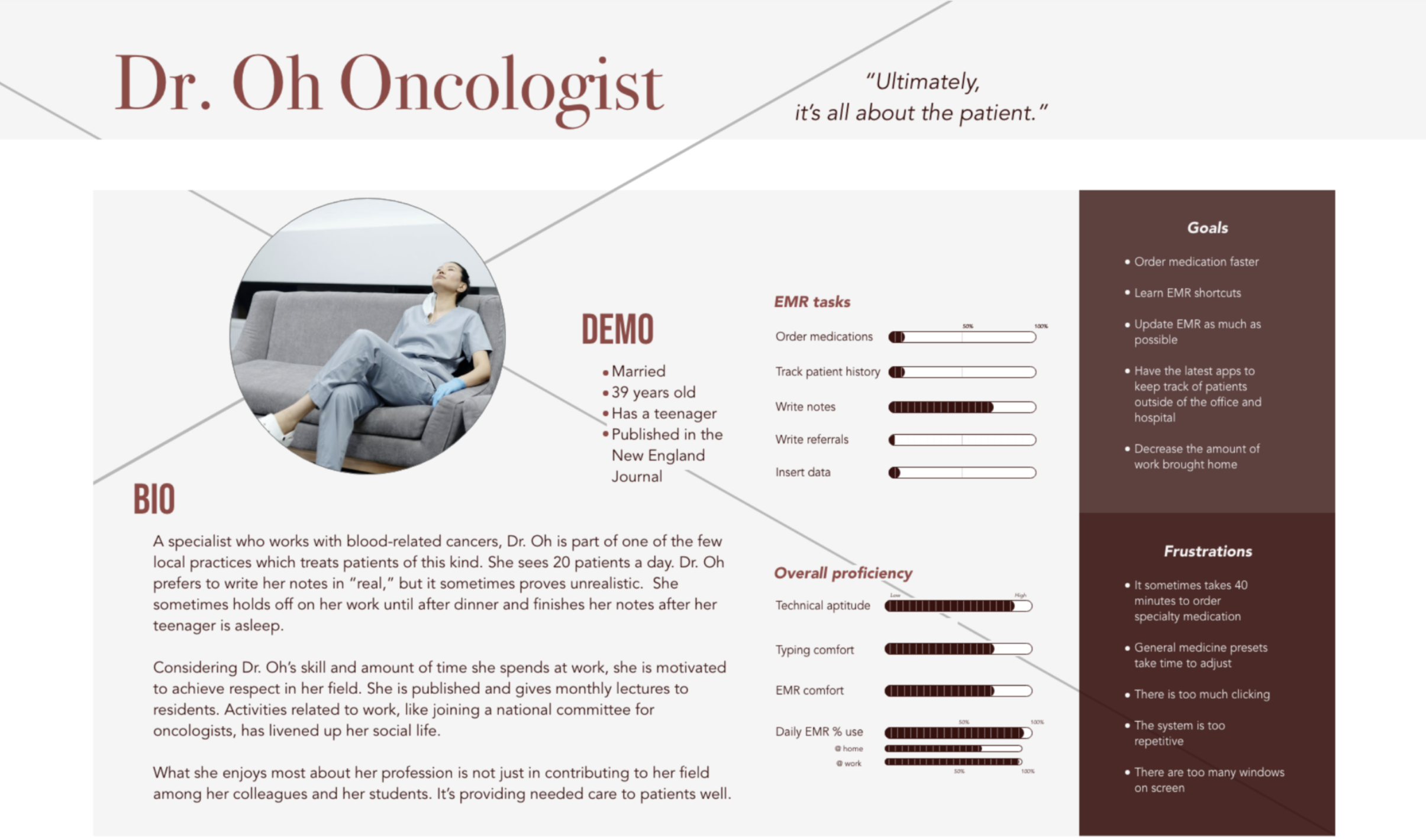
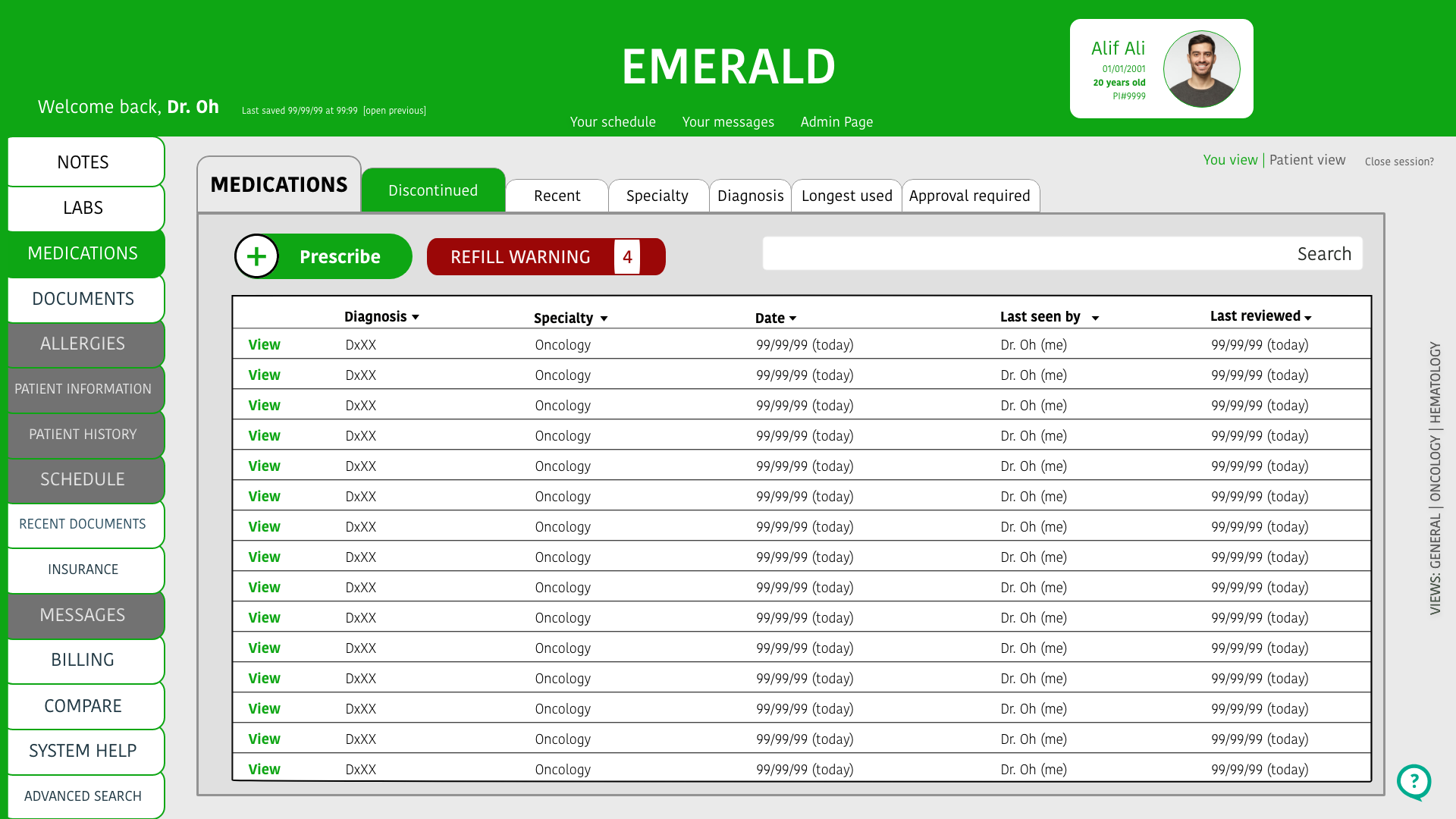
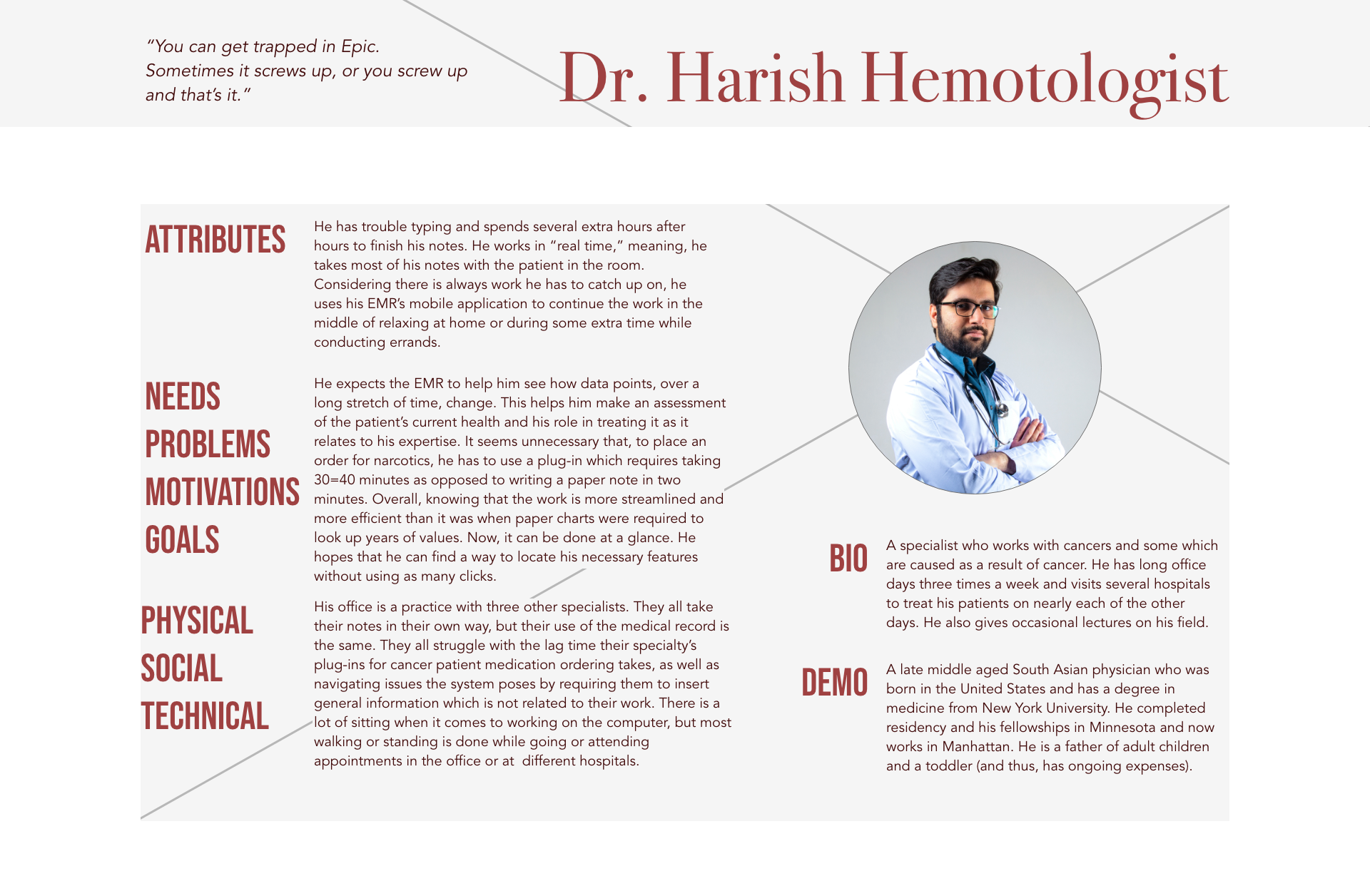
Key Persona: Dr. Oh Oncologist is proficient in modern tech, but spends far too much time on the ancient technology at work.
Dr. Oh’s goals:
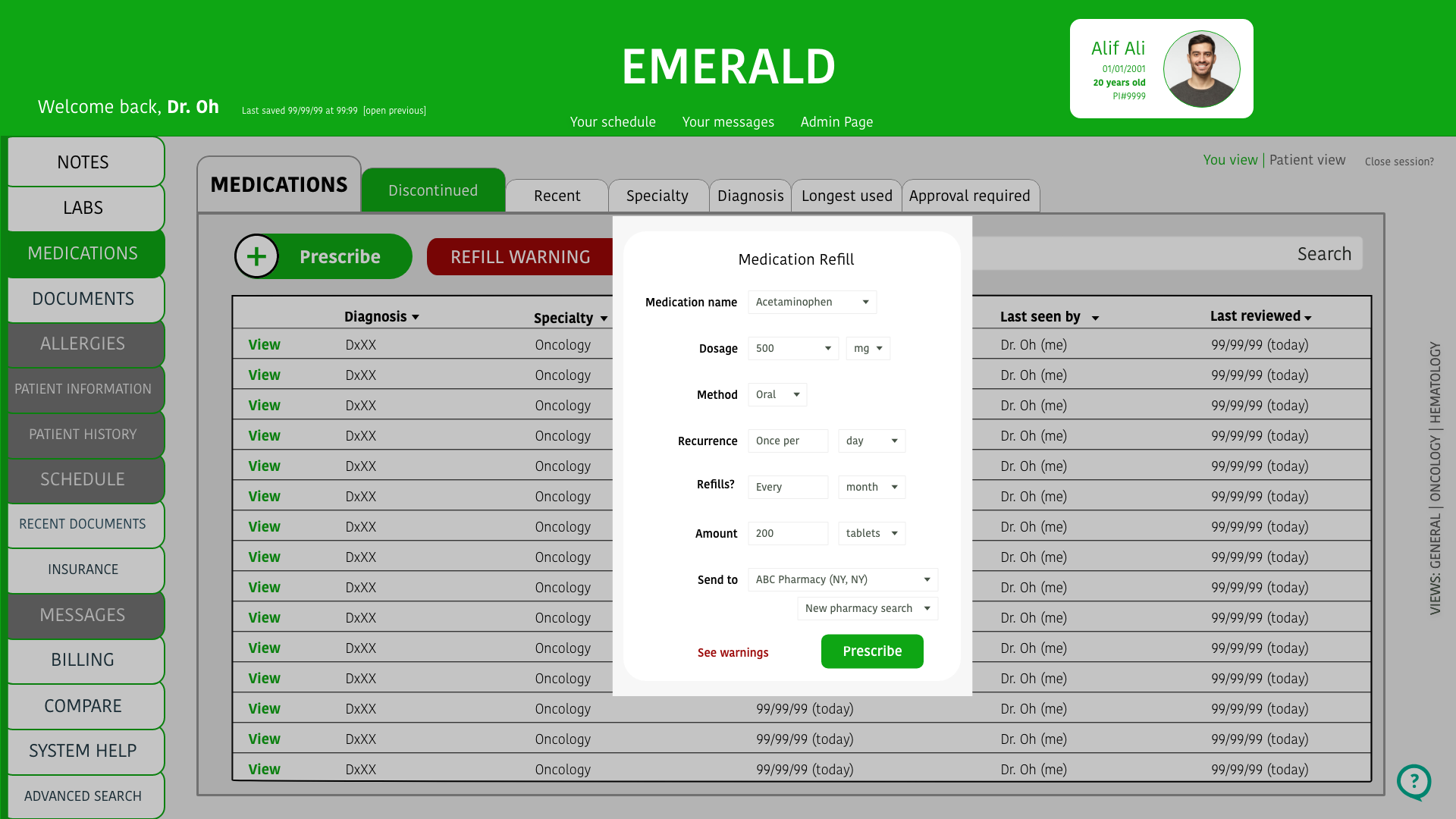
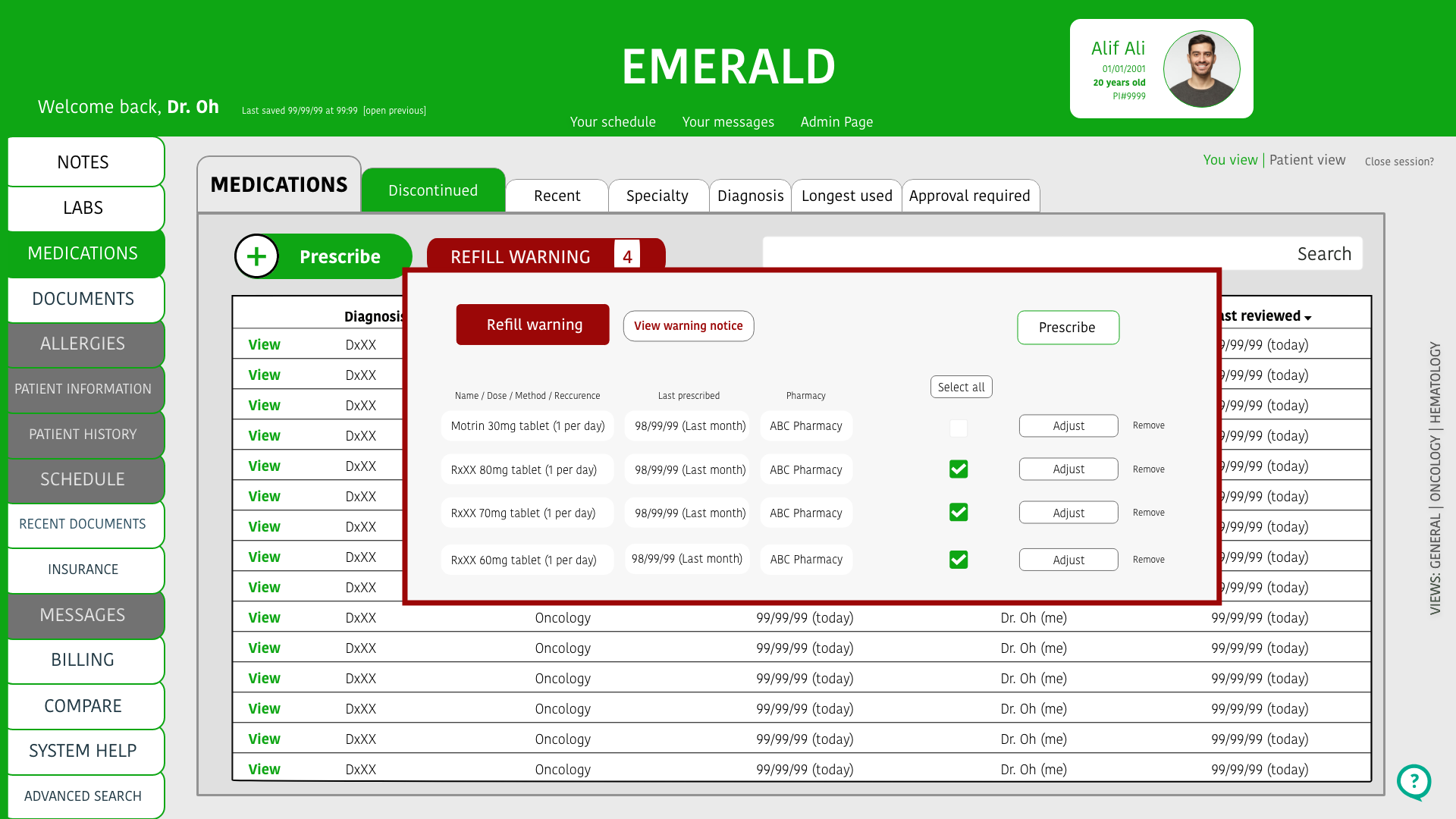
- Order medication faster.
- Learn EMR shortcuts.
- Update EMR as much as possible.
- Have the latest apps to keep track of patients outside of the office and hospital.
- Decrease the amount of work brought home.
Dr. Oh’s Frustrations:
- It can take 40 minutes to order specialty medication.
- General medicine presets take time to adjust.
- There is too much clicking.
- The system is too repetitive.
- There are too many windows on screen.
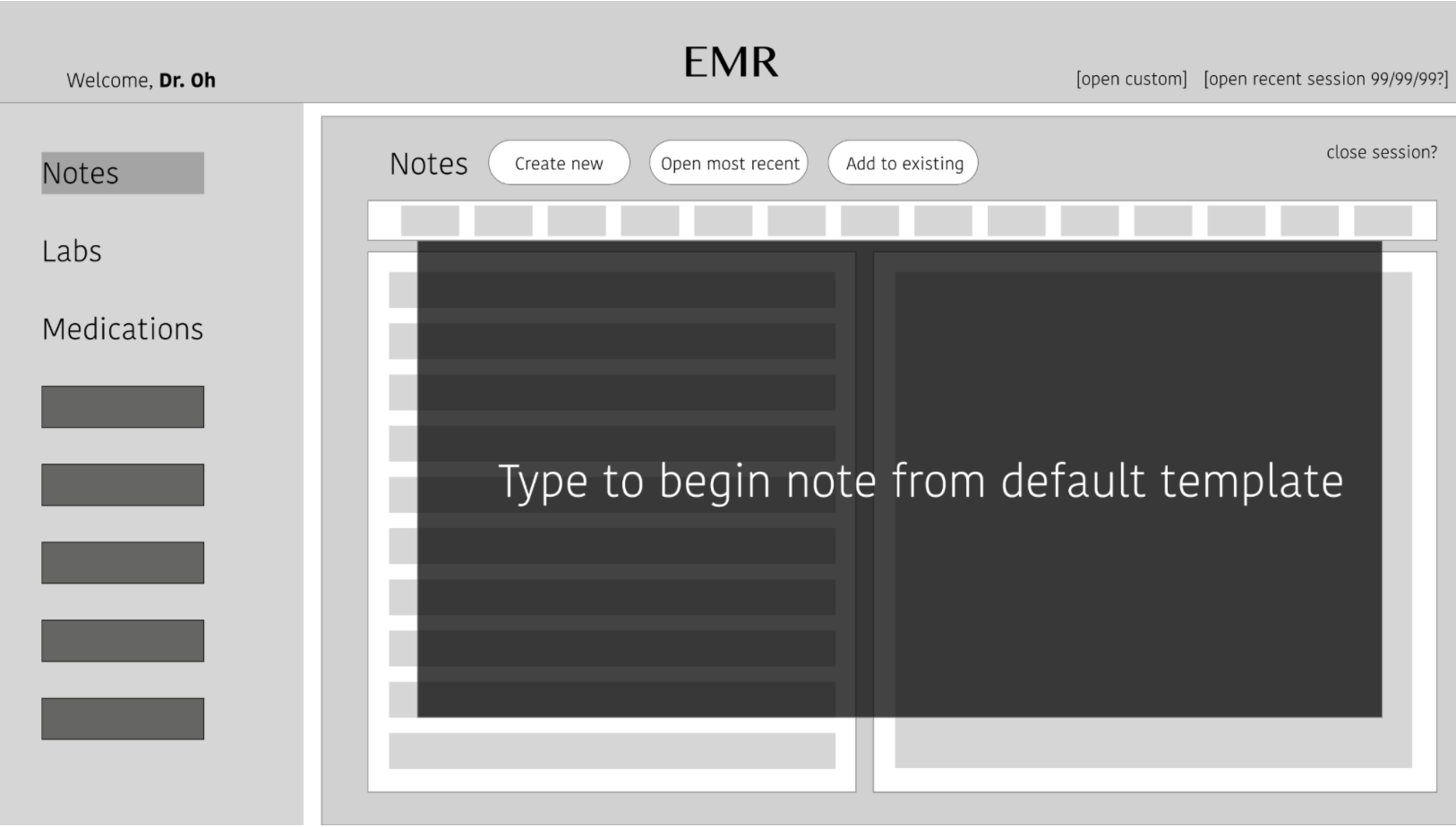
Sketch Testing
Notes tab and the interface shows a blank note to fill in. This feature is for those times a few ideas need to be jotted or for any impression which may not warrant a formal template to fill out. During my “guerrilla” testing, participants found this a useful idea.
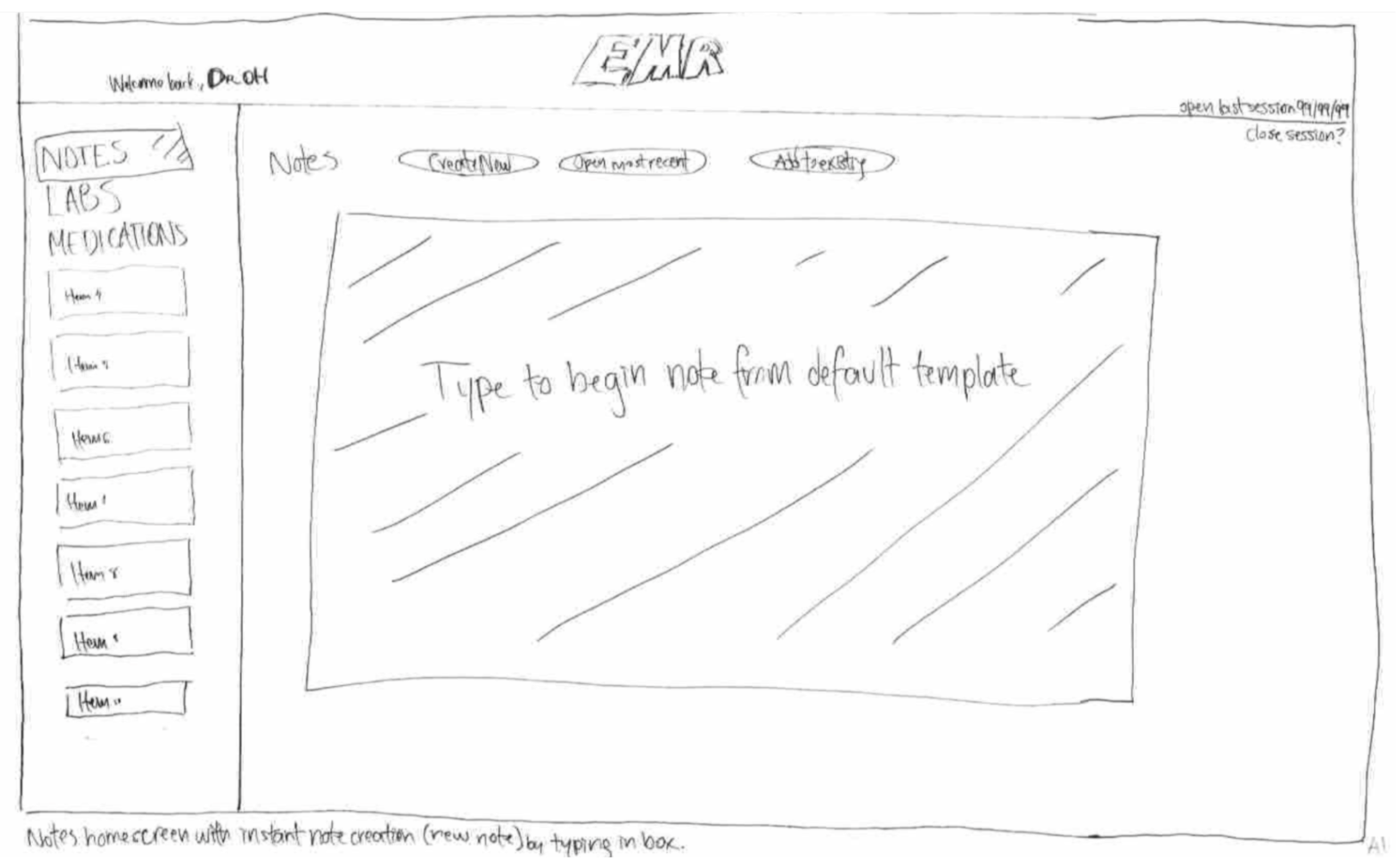
Sketch for guerilla testing: Instant Notes feature
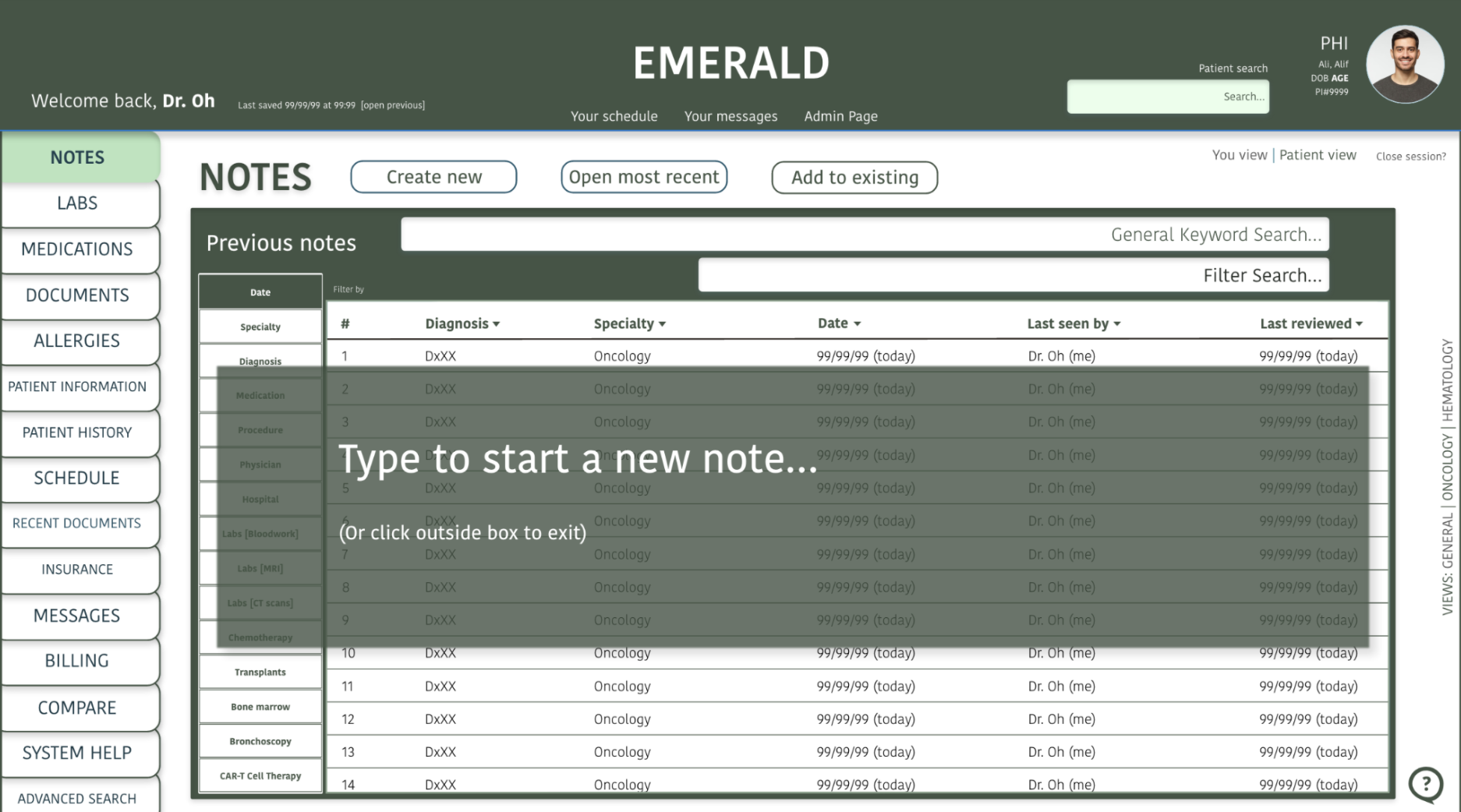
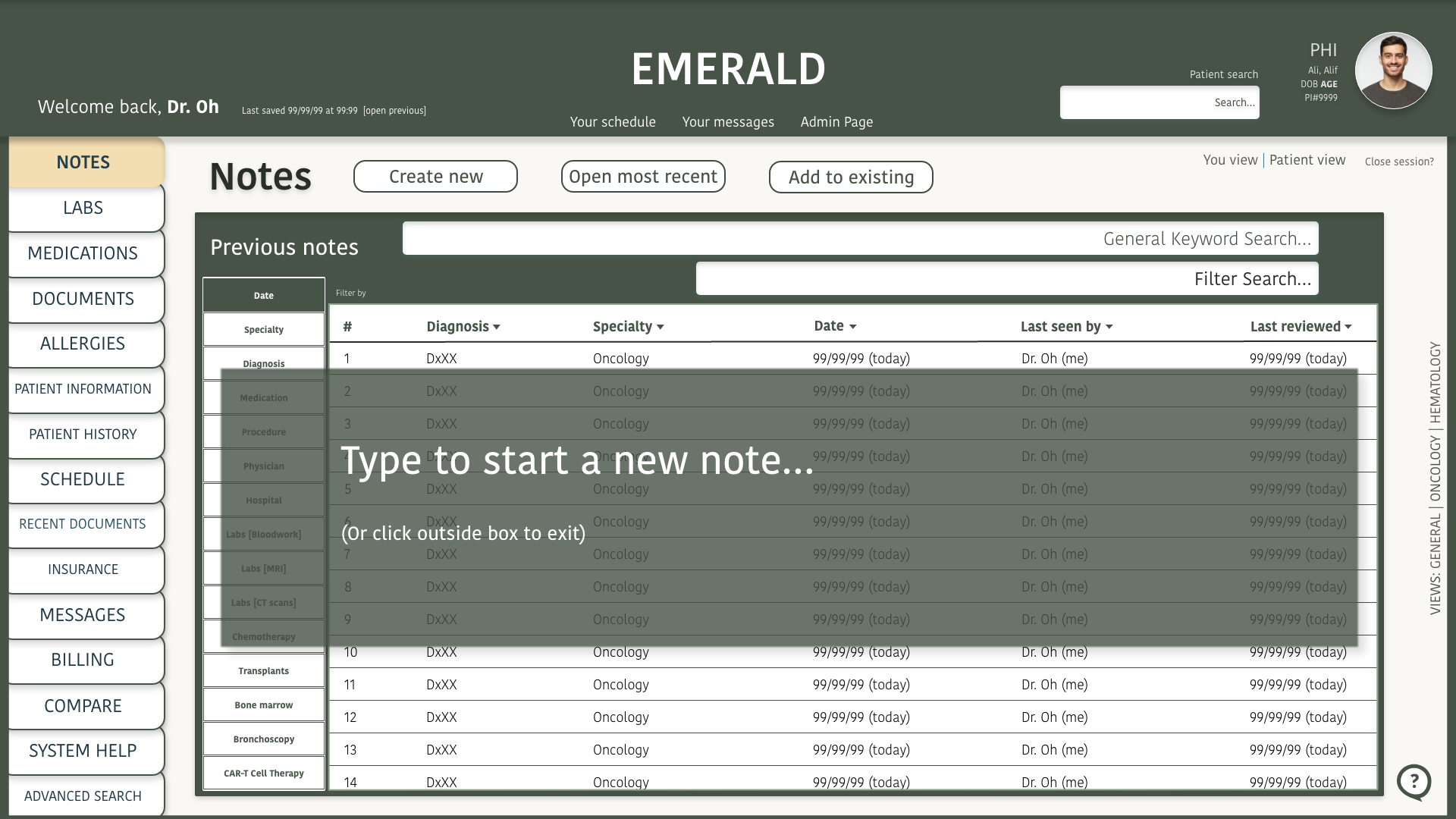
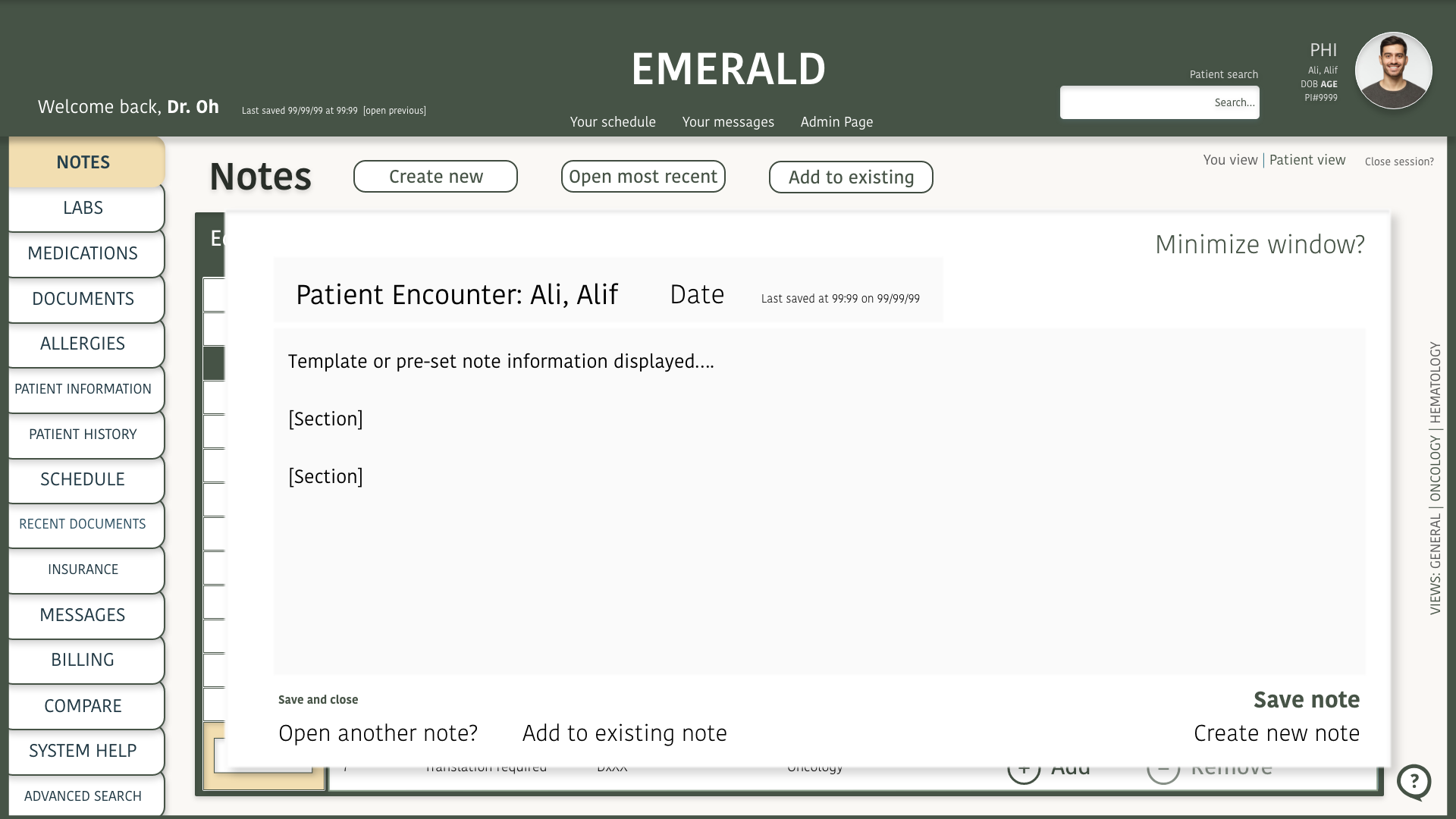
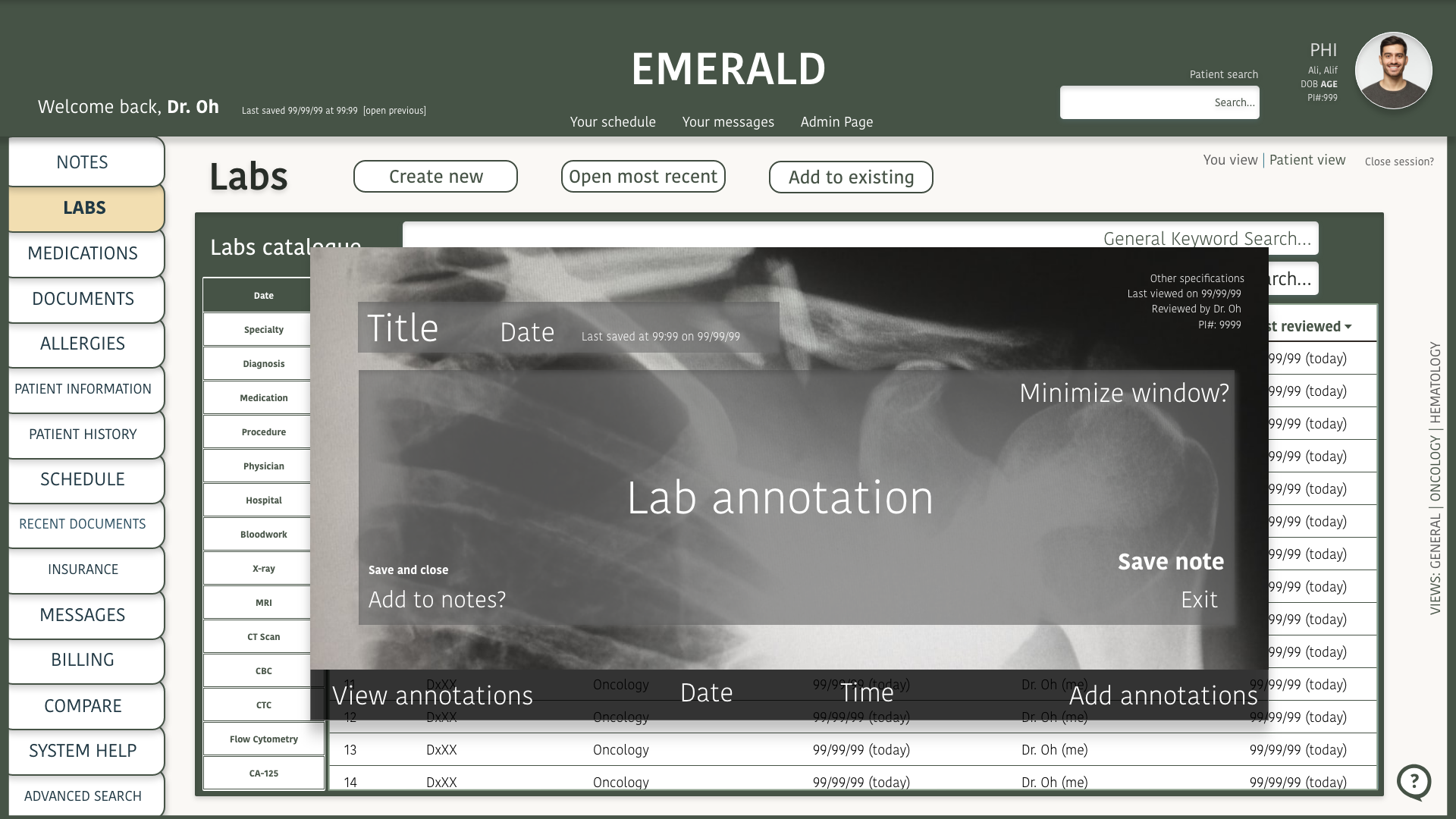
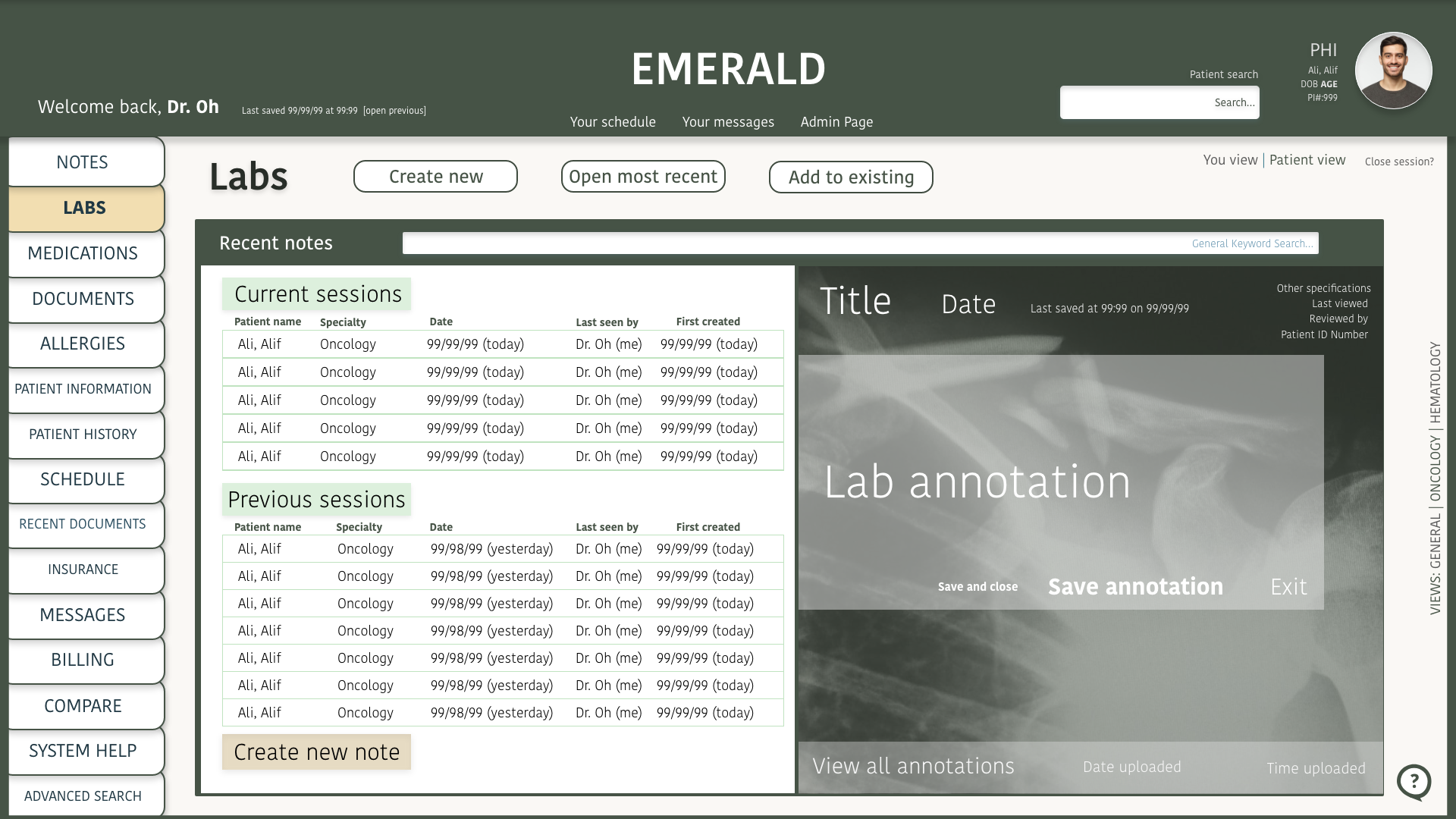
High Fidelity
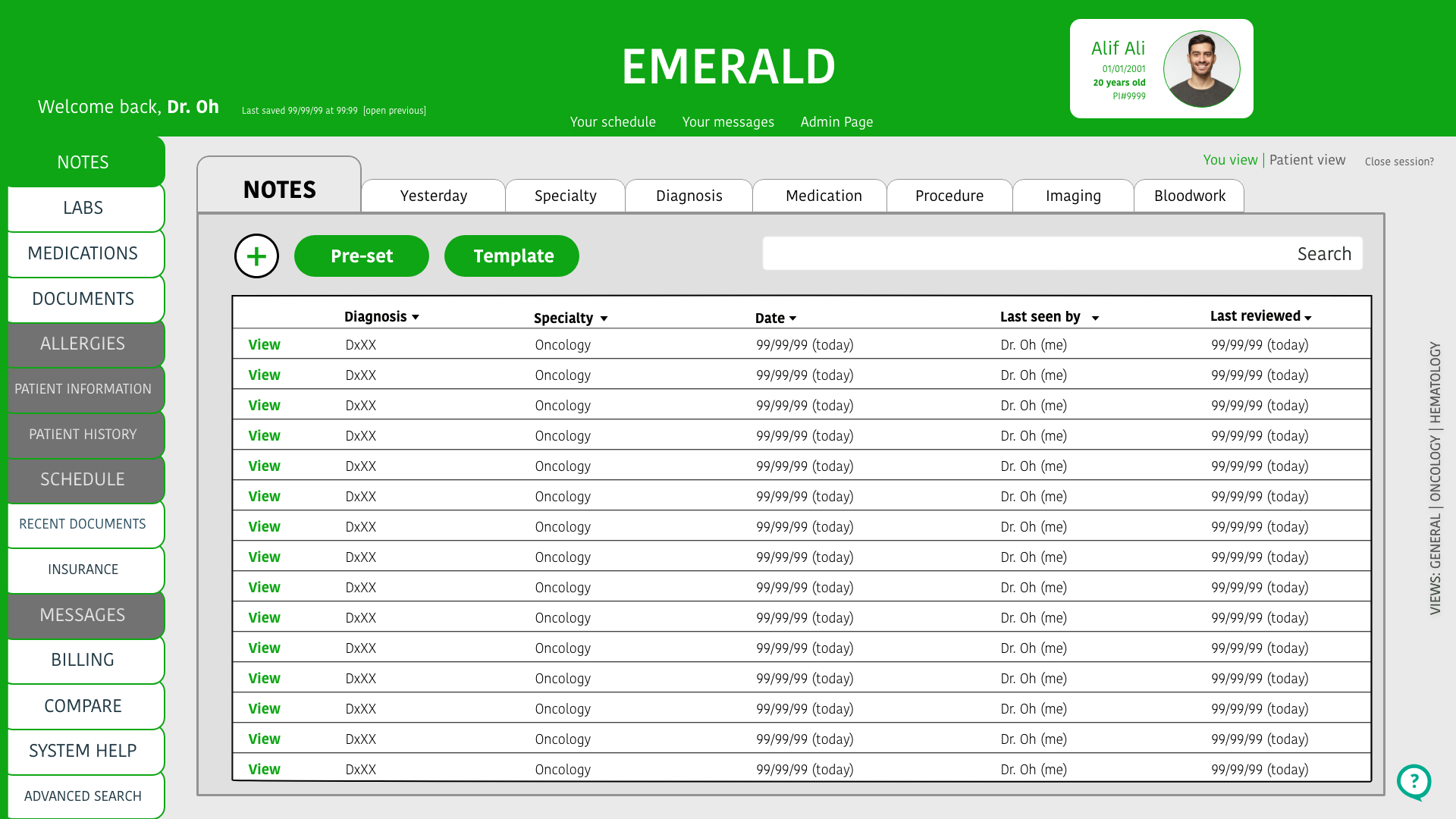
In my final iteration, I removed the feature.
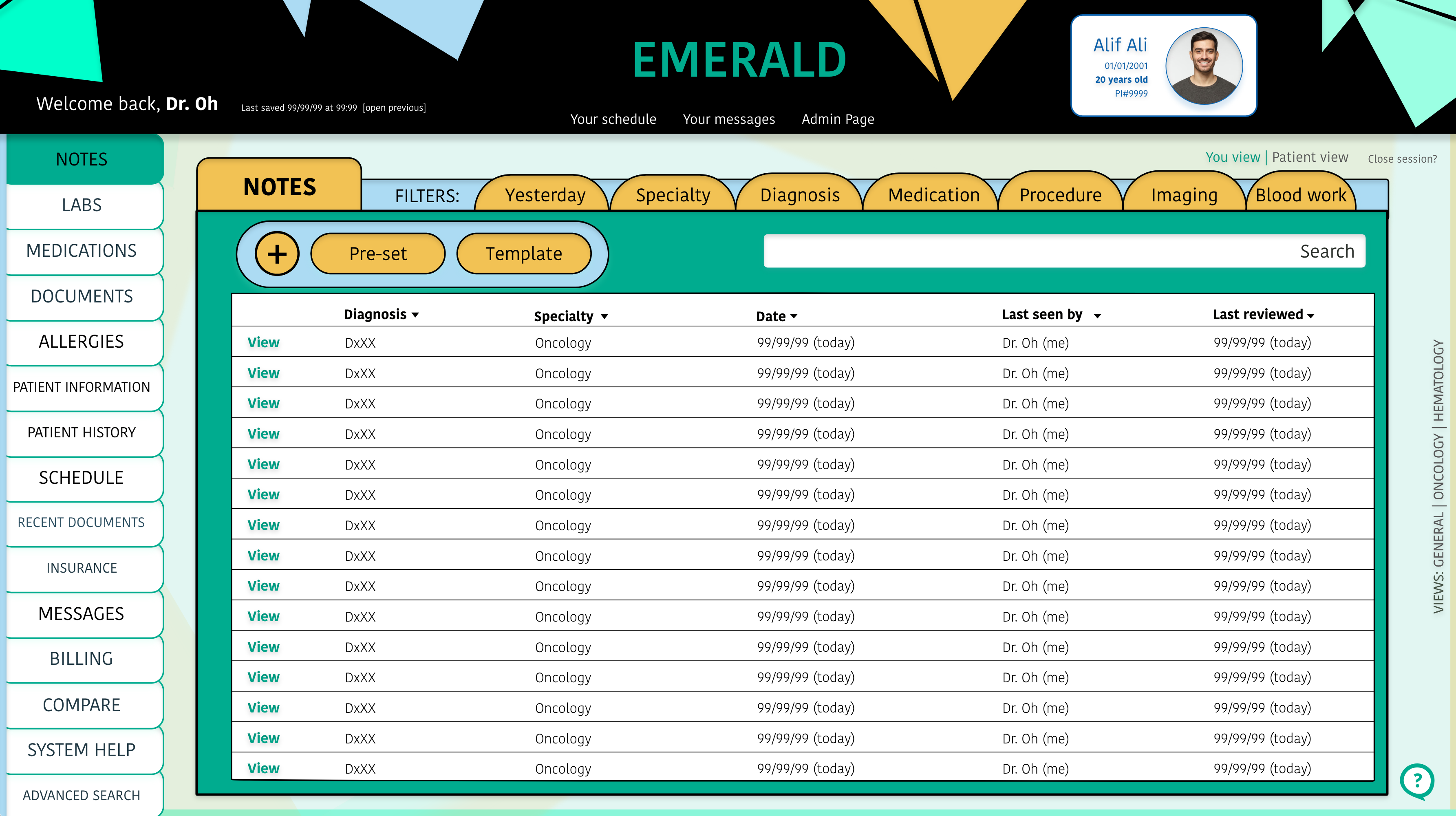
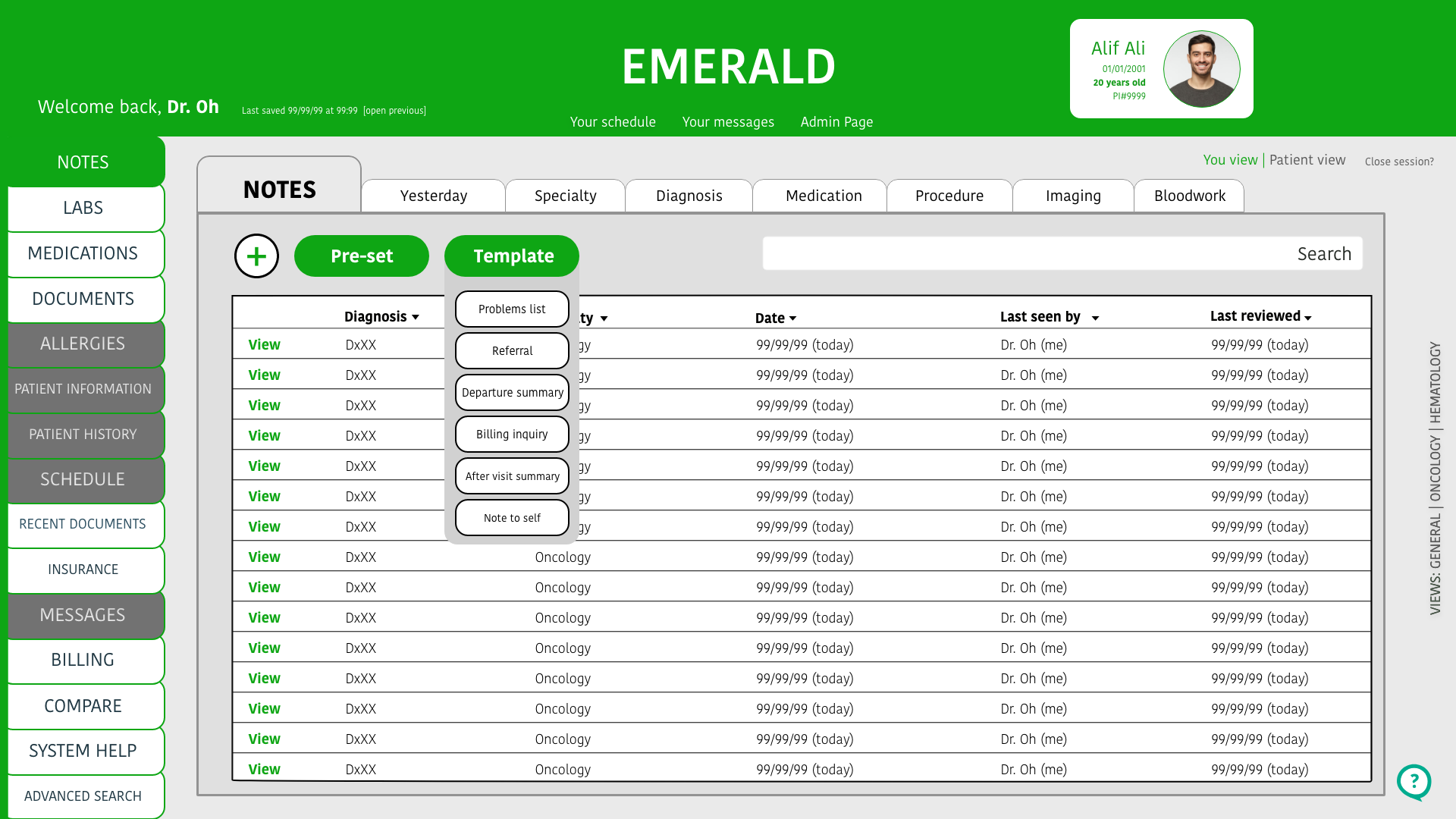
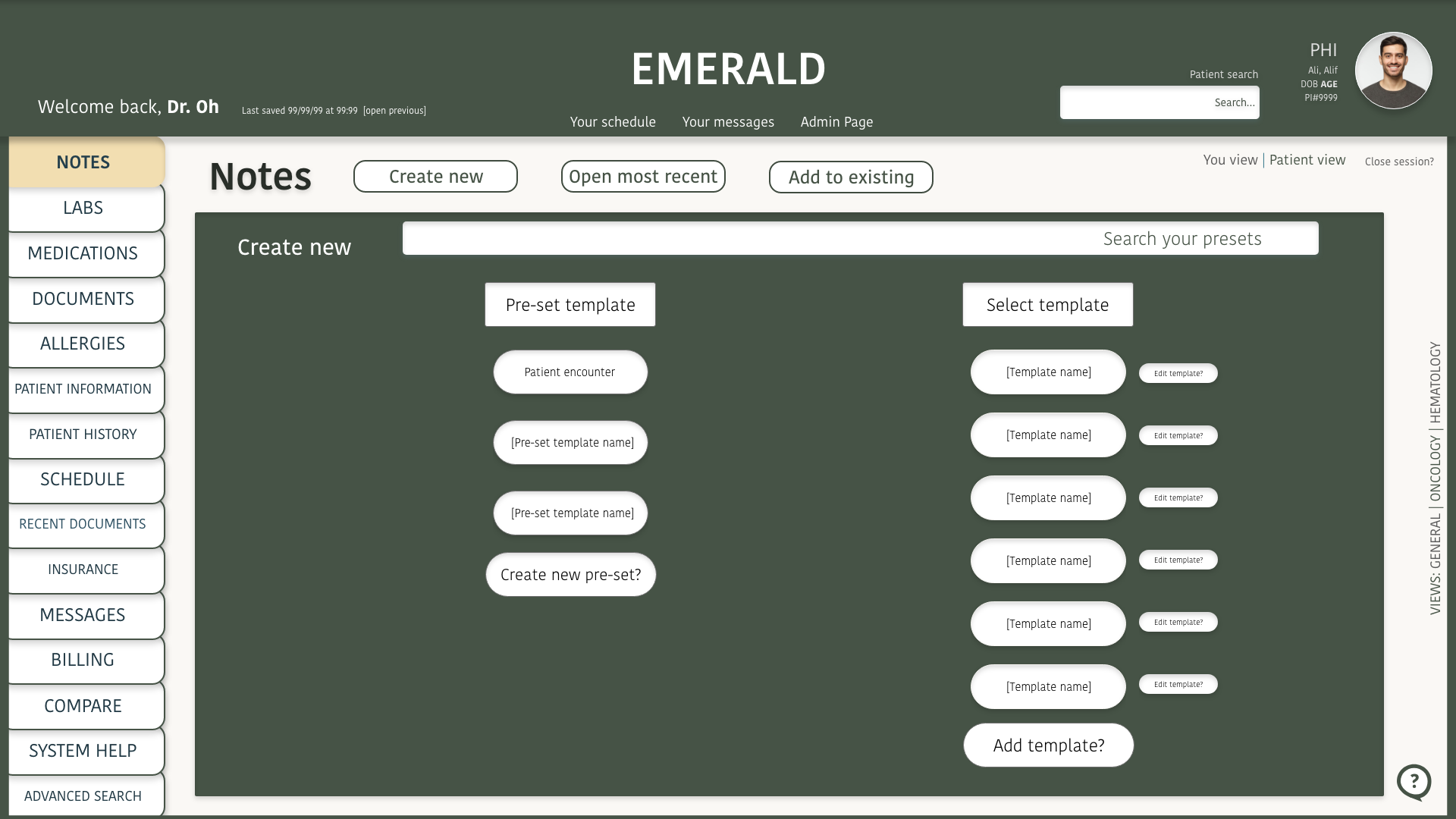
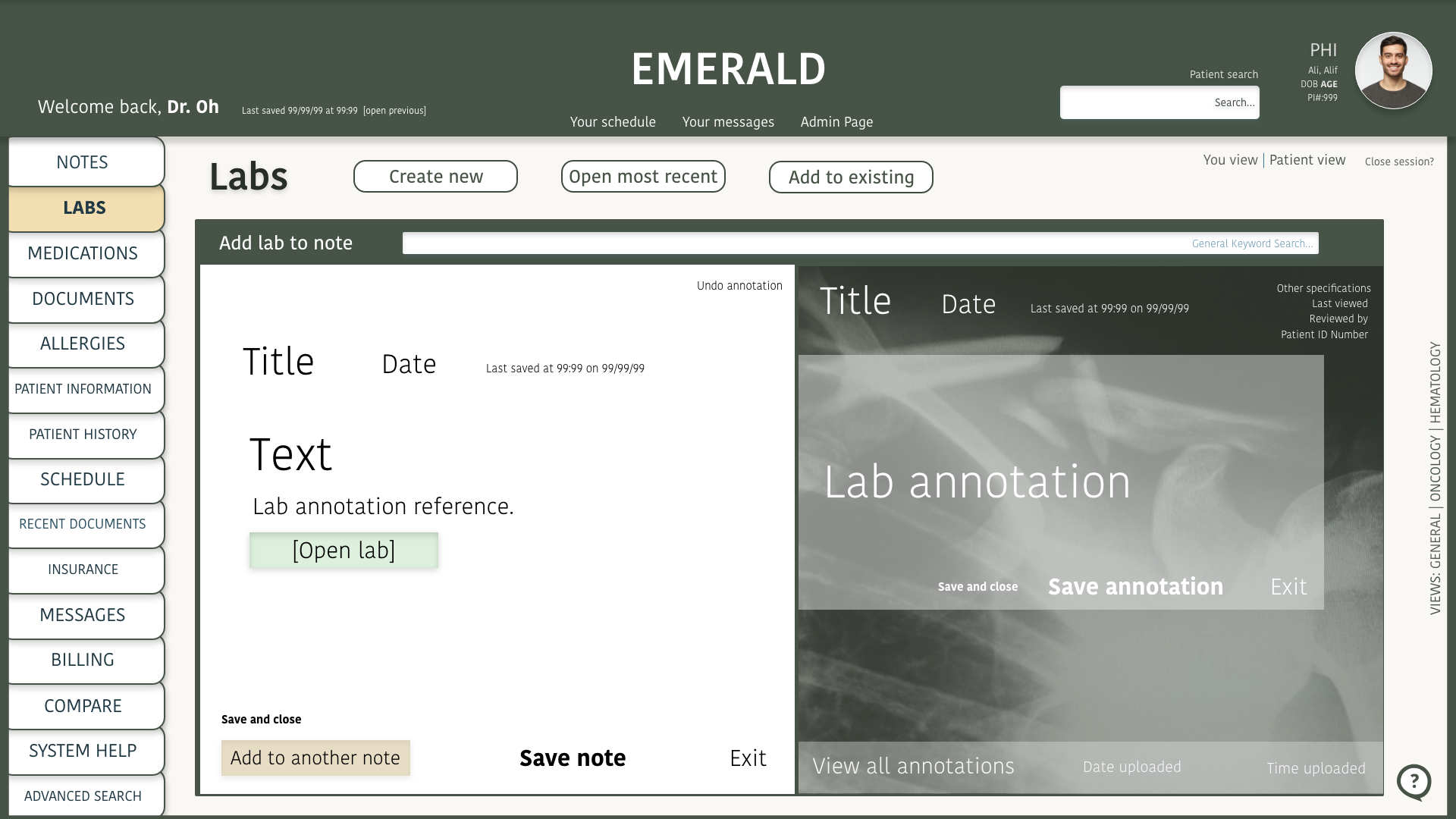
A different idea for making the note writing experience faster was to add a plus sign on the page. Clicking on this would mean adding a new note. I added the option to select a previously used customized note (pre-set) or a template from Emerald.
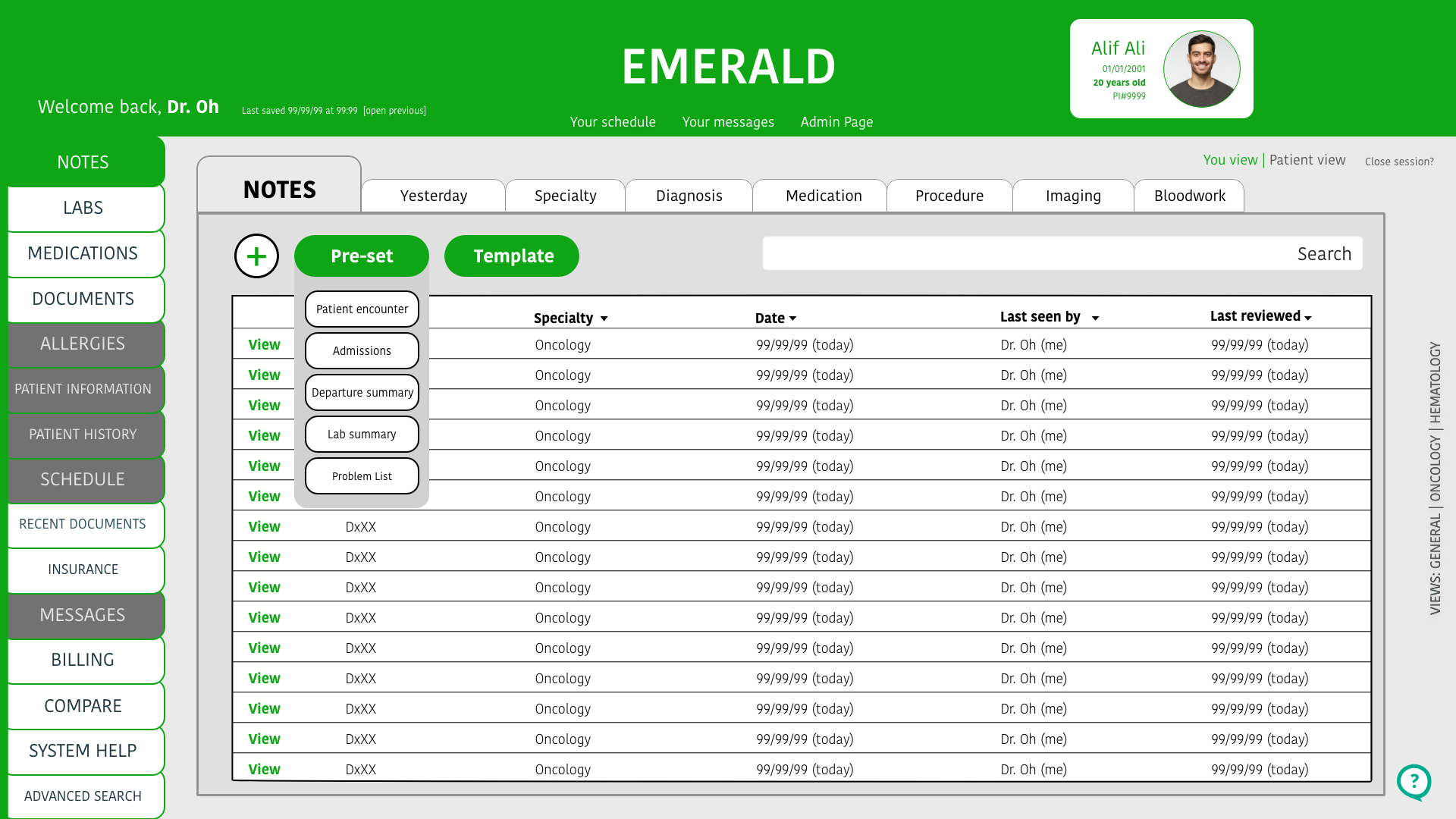
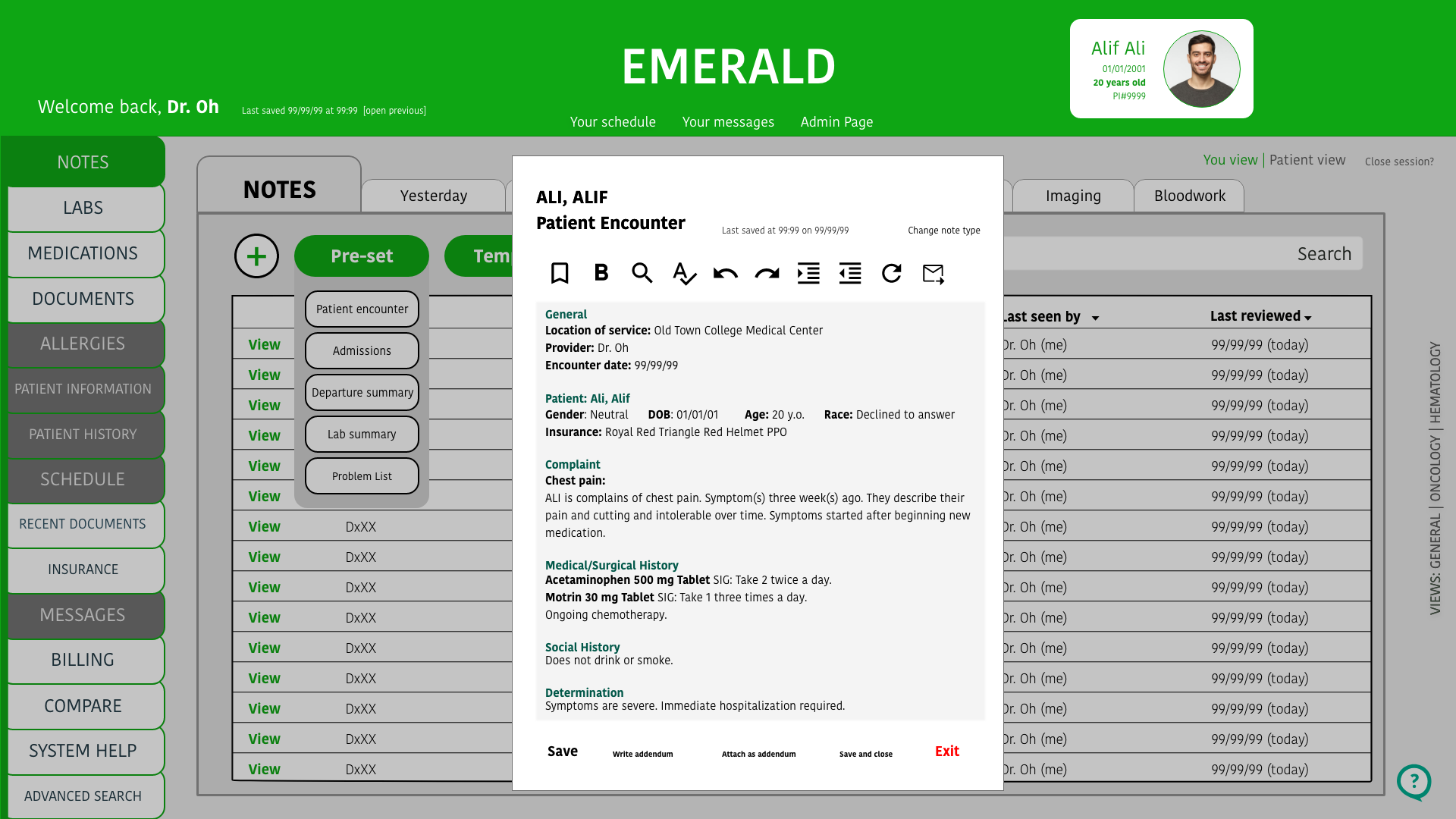
It was recommended to remove “pre-set” and “template” and only keep the plus sign. The plus sign is intuitive enough and made the other options – so after clicking the plus sign, a user is then prompted to choose which kind of note they want to move forward with. Users found this intuitive and it fit their demand for personalizing their notes.